Horse Caudal Pectoral Strains and Tears
Caudal Pectoral Strains and Tears
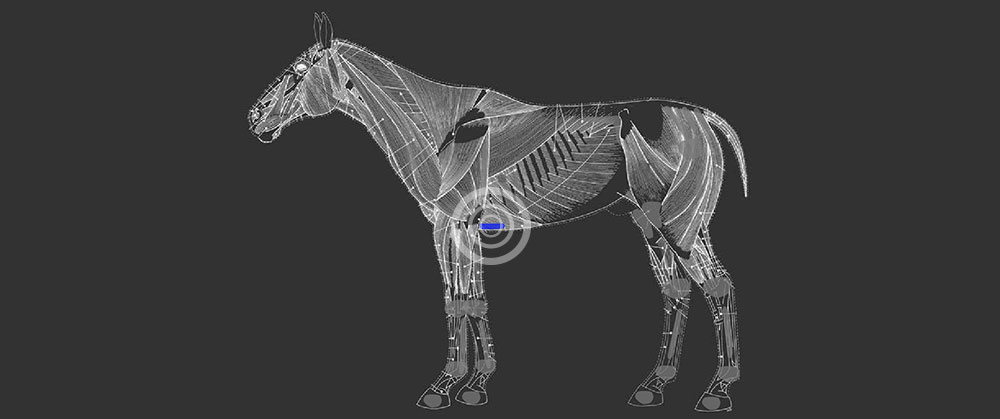
On palpation of an injured caudal pectoral muscle the region feels firm and unyielding to palpation and pressure and unresponsive to stretching initially. The horse commonly reacts to tightening of the girth when saddling and there is a noticeable shorting of the stride on walking off after saddling which improves with slow trotting exercise. There is commonly a secondary associated hypertonicity of the psoas muscle group due to these muscles having a similar nerve network.
The acupuncture work up is very effective in differentiating between a strain in the muscle and secondary hypertonicity from another region of the body. Proper treatment can then be initiated in which acupuncture can be of primary benefit to the region. Acupuncture is used to restore the chi and blood stagnation locally and to reduce the caudal pectoral muscle hypertonicity and pain. By doing this the muscle spindles are reset which allows for muscle lengthening and a reduction in hypertonicity Liniments and or ultrasound therapy are used locally to increase heat and reduce hypertonicity to allow the region to heal with reduced scar tissue, this reduces the chance of re injury in the region by enhancing elasticity of the region.
Passive stretching of the region is another ongoing therapy which can greatly enhance the results. For this injury the affected forelimb is picked up, flexed and drawn forward to stretch the caudal pectoral muscle, this can be done both before and after exercise daily. The use of thick girth covers can help spread the stress of the girth on the caudal pectoral region and it is recommended that galloping be reduced as to give the strain or tear the chance to recover.
It is common however that after the strain in the pectoral muscle has resolved, there is still remaining hypertonicity in the pectoral muscles. This is due to a dysfunction in the reflex arch associated with the muscle, due the presence of inflammation in the sensory and or motor nerve. It has therefore been found that the use of nerve anti-inflammatorys such as DMSO as used by nasogastric tube or injected locally can help resolve this inflammation and allow the muscle to return to it’s proper resting state.

